How to eat if you take a GLP-1 (Ozempic, Wegovy, Mounjaro, Zepbound)


How to eat if you take a GLP-1 Medication
Understanding Nutrition on GLP-1s
Over the past few years, I’ve immersed myself in the evolving science and clinical experience surrounding GLP-1 receptor agonists —medications you may know as Ozempic, Wegovy, Mounjaro and Zepbound. Originally developed for managing type 2 diabetes, these medications are now making headlines for their broader impact on weight, metabolic health and cardiovascular health.
Their use is rising rapidly, and with good reason:
- These medications have been shown to reduce blood sugar, improve fatty liver, GERD, sleep apnea, osteoarthritis, blood pressure, triglycerides, major adverse cardiovascular events, and even show potential benefits for conditions like alcohol use disorder (Mozaffarian et al., 2025; Gigliotti et al, 2025).
But weight loss isn’t just fat loss. Without a thoughtful nutrition and lifestyle strategy, GLP-1 users risk losing muscle and bone mass as well. In any medication that reduces appetite, nutritional adequacy becomes a concern.
It’s important to understand both the benefits and the risks associated with these medications.
Why GLP-1 Medications Are Gaining Attention
GLP-1s (glucagon-like peptide-1 receptor agonists) help regulate appetite and blood sugar by:
- Reducing hunger
- Enhancing satiety
- Improving insulin secretion and slowing gastric emptying
- Reducing food cravings and “food noise”
My role as a dietitian in GLP-1 use
As a registered dietitian and nutritionist, I work with many clients taking Ozempic, Wegovy, Saxenda, and Mounjaro [For a list of the GLP-1 medications, see Figure 1 of this article]. My role is to assess their nutritional status, optimize their intake, and help them feel nourished—not restricted—on these powerful medications.
We talk about things like:
- How much protein do you actually need?
- How can we protect your muscle mass, bone mass and metabolism?
- What can you eat when your appetite is lower or unpredictable?
- How to get adequate nutrition in ways that work with current preferences and skills?
- How can you eat enough without feeling overwhelmed or disconnected from your body?
Whether you’re taking these medications, considering them, or simply feeling confused about all the hype, I want to open up the conversation and help make it less overwhelming, and quite frankly, shame-free.
Before I attempt to cover this rapidly evolving topic, I want to acknowledge a few important points:
- I live in a smaller body. I don’t experience micro-aggressions in this world about my body and have never walked a mile in your shoes.
- I do not take a GLP-1 myself but have worked with hundreds of people who have.
- I am not being paid to explain this medication. I have no vested interest in whether you take this medication.
- I am neither for nor against this medication. I am agnostic about your use of GLP-1s. However, I feel strongly that people need to be informed about both the risks, benefits, and limitations of this (or any) medication that they use, which is part of the “informed consent” process between you and the prescribing professional.
- This is not a comprehensive product monograph and this is not a substitute for medical advice. The GLP-1 medications are not appropriate for all people.
Topics This Post on GLP-1s Covers:
- What are GLP-1 medications and how do they work?
- How common is GLP-1 use?
- Research-backed benefits of GLP-1s
- A note on weight plateaus
- Common client experiences
- Key nutrition concerns for GLP-1 users
- GLP-1s and “food noise”
- What happens when I stop taking GLP-1 medications?
- Is taking a GLP-1 the “easy way out”?
- Final thoughts & nutrition tips.
What are GLP-1 Medications and how do they help?
GLP-1 stands for Glucagon-like peptide 1 receptor agonists and combination medications, which I will refer to as GLP-1s, are changing the treatment of obesity (a chronic, relapsing and remitting condition that impairs health) and metabolic health concerns including diabetes, prediabetes, MASLD, and cardiovascular disease risk.
GLP-1s amplify a hormone our bodies naturally release during digestion. This hormone decreases hunger, increases satiety. slows digestion, and enhances insulin secretion—key mechanisms for blood sugar and weight regulation.
Medications like Ozempic and Mounjaro (approved for type 2 diabetes) and Wegovy and Zepbound (approved for weight management) amplify these effects. GLP-1s essentially put your fullness signals on “steroids,” allowing you to feel full sooner and for longer.
How Common Is GLP-1 Use?
GLP-1s are becoming more common. In the U.S., about 6% of adults currently use GLP-1s, and 12% have used them in the past (2024 data) (Mozafariun 2025).
Research-Backed Benefits of GLP-1s
In clinical trials, GLP-1s lead to weight reductions of 5–18%, up to 25% after about 56–72 weeks of use. While real-world results may be slightly less, the improvements go beyond weight:
- Lower blood sugar, blood pressure, and triglycerides
- Reduced waist circumference and sleep apnea symptoms
- Better health-related quality of life
- Fewer major cardiovascular events
- Reduced progression of fatty liver disease and chronic kidney disease—even in the absence of weight loss (Mozaffarian et al., 2025).
Greater improvements are observed at higher doses (Mozafarrian et al 2025; Sievenpiper 2026).
Table 1 of this article summarizes the results of industry-sponsored randomized controlled trials. According to researchers, weight reduction is quicker in the first 6 months, and slows after that, plateauing at 12-18 months.
A Note on Weight Plateaus
Our bodies resist weight loss and have many biological adaptations to resist sustained weight loss. At some point, a weight loss plateau is expected. Weight loss typically slows or plateaus by 12–18 months while using a GLP-1. When losing weight, our bodies naturally adapt; our intake is reduced. As we lose weight, we also reduce how much energy we expend. When this happens, our intake matches our reduced energy expenditure, which creates what is known as our “best weight” (Hall et al, 2024).
This is important context when managing expectations of “results” from taking GLP-1s as well as addressing the internalized weight bias that many of us hold after marinating in diet and weight-biased medical culture.
What Clients Are Telling Me about their experience with GLP-1s
Client responses to GLP-1s vary widely:
- Some experience little to no appetite or weight change—possibly requiring dose adjustments.
- Some feel fantastic with reduced cravings and appetite.
- Some lose their appetite entirely, struggling to eat more than once or twice a day—raising risk of malnutrition.
- Others are unable to tolerate GLP-1s and stop due to persistent side effects.
These experiences are supported by research. Some people experience minimal weight reduction with GLP-1s, while others have weight reductions >30% of their weight (Mozafarriun et al, 2025).
The takeaway? There’s no one-size-fits-all experience. That’s why personalized guidance is so important.
Key nutrition concerns for GLP-1 users
What this midlife dietitian focuses on when working with someone taking a GLP-1
As a dietitian, there are many things I consider when working with someone who is taking a GLP-1 medication. These concerns can be partially mitigated by an intentional lifestyle program, particularly around food.
-
Supporting Digestion
Digestion is already a challenge for women around menopause. Digestive side effects of GLP-1s include nausea, bloating, vomiting, constipation, diarrhea, belching, indigestion and more, outlined in Figure 3 of this article and Table 2 of this article.
Mild to moderate side effects are often observed in the early weeks (~first 6) of medication use and during dose escalation. Increasing the dose slowly over time helps to minimize the frequency and severity of GI symptoms.
We see these side effects for a few reasons: GLP-1s delay how fast our stomachs empty which can lead to bloating, fullness and nausea. This experience is influenced by what you eat, with higher fat meals making this side effect worse. GLP-1s also activate several areas of our brain involved in weight regulation, appetite and nausea.
Nausea is the most common GI side effect. It often occurs in the morning and/or after longer periods without eating.
Strategies that help manage nausea:
- Eat a small breakfast. Then eat smaller, more frequent meals (every 3–4 hours) with smaller portions than usual. Stop at first signs of fullness.
- Stopping eating 2-3 hours before bed can significantly reduce acid reflux caused by delayed gastric emptying (Almandoz 2023).
- Limit foods high in fat and fiber during periods of nausea. Limit spicy foods.
- Stay well hydrated (2–3 L/day). Maintaining adequate hydration is critical to prevent acute kidney injury as well as heart palpitations. Moderate use of carbonated beverages.
- Use ginger, peppermint, or acupressure bands for symptom relief
Optimizing fat intake can also be helpful for managing steatorrhea (oily stools – reduce fat intake). Rapid weight loss increases gallstone risk. Maintainin a minimum intake of fat of 25-60 g/day is recommended to stimulate gallbladder emptying, and therefore a reduced risk of gallstones (Sievenpiper 2026).
Strategies on how to manage these and other side effects are described in more detail here: Figure 3 of this article and Clinical Recommendations to Manage Gastrointestinal Adverse Events in Patients Treated with Glp-1 Receptor Agonists.
-
Protecting Muscle & Bone Mass
About 20%, up to 40% (Spreckley 2026) of total weight lost can come from muscle tissue—something especially concerning for women in perimenopause or menopause, who are already losing lean mass with age.
After the age of 30, we begin to lose lean muscle mass at a rate of 3-8% per decade. This rate may be even faster as we age, especially after the age of 60 years. Without intentional strength training and nutrient targeting, we can lose up to 30% of our muscle mass between the ages of 50-70 years. For more information, read Muscle tissue changes with aging.
Focusing on scale weight as your marker of progress can miss the mark on improved body composition. In fact, the goal of GLP-1 use is to focus on physical health, mental health and well-being, rather than body weight alone (Mozafarriun et al 2025).
Lean body mass is affected by the degree of calorie restriction, rate of weight loss, optimal protein intake and the presence/absence of strength training. Low protein intake due to reduced appetite may also contribute to muscle loss and increased risk for sarcopenia especially among those with older age, sedentary behaviour and a lack of resistance/strength training.
More recent guidelines recommend screening for sarcopenic obesity, which is the loss of muscle despite higher body weight, especially in older adults (Spreckley 2026; Sievenpiper 2026). Prior to starting a GLP-1 medication, baseline testing such as handgrip strength or chair-stand testing is now suggested (Sievenpiper 2026).
What is a reasonable rate of weight loss while on a GLP1?
According to a 2026 paper, “faster is not always better”. Losing weight too quickly could be a red flag for muscle loss and bone mineral density. Excessive weight loss was defined as >1.5 kg/week or >3.3 pounds/week (Sievenpiper 2026).
Weight loss that exceeds 5% of total body weight within a month is a trigger for evaluation (Schweitzer 2026). A reduction in GLP1 dose or a pause in dose escalation to prioritize lean body mass preservation.
A suggested rate of weight loss is 0.5 – 2 pounds/week (Schweitzer 2026).
What helps mitigate loss of lean body mass:
- Protein: Aim for 1.2–1.6 – 2.0 g/kg body weight/day (never less than 0.4–0.5 g/kg). An adjusted body weight may be used here. One article outlined 25-30% of a 1600 kcal diet, which works out to 100-120 g/day of nutritional protein (Sievenpiper et al 2026).
- Prioritize whole-food protein sources: dairy, eggs, seafood, lean meats, poultry, legumes, tofu, Greek yogurt, and high-protein snacks. As appetite is often reduced on GLP-1s, getting enough protein can be challenging.
- Distribute protein intake throughout the day, starting with breakfast, for maximal protein synthesis.
- If there is a history of kidney stones, specific adjustments to the type of protein consumed are recommended.
- Resistance training 3x/week plus 150 minutes/week of moderate cardiovascular activity (you can talk but can’t sing).
Focus on body composition, not scale weight.
Interested in this topic, you can read more in several articles: fat loss vs weight loss, the effects of medically induced weight loss on skeletal muscle, changes in fat-free mass during significant weight loss: a systematic review, and fat-free and skeletal muscle loss with GLP-1 treatments.
3. Preventing Nutritional Deficiencies
People struggling with their weight are already at risk of suboptimal dietary patterns if they have pursued or are pursuing intentional weight loss because of reduced food intake and sometimes, insufficient calorie and nutrient intake. Some are struggling with their intake of ultra-processed foods. Some struggle with nutrient absorption, distribution, metabolism, or excretion.
While taking a GLP-1, there is a significant reduction in appetite and energy intake, between 16-39%; these changes are thought to be related to changes in cravings, hunger and fullness (Mozafarriun et al 2025).
Reduced appetite = reduced intake = increased risk of missing key nutrients like:
- Protein
- Iron, calcium, magnesium, zinc, potassium, choline, folate.
- Vitamins A, D, E, K, B1, B12, and C
Eating less often leads to nutritional inadequacy even when weight loss is “successful”. One study found that over 90% of GLP1 users failed to meet requirements for Vitamin D, potassium and choline (Spreckley 2026).
Symptoms like hair loss, fatigue, flaky skin, or bruising, muscle weakness, poor wound healing may indicate insufficiency (Mozafariun et al 2025).
Supportive strategies:
- Prioritize nutrient-rich, minimally processed meals (veg, fruits, whole grains, legumes, lean proteins, nuts, seeds) and fluids so that the foundation of their diet is nutritionally adequate. I work with my clients on strategizing and personalizing this information to fit their skills, capacities, and their life.
- Schedule meals even if not hungry (aka mechanical eating)
- Focus on hydration, especially with nausea or low intake.
- Add in targeted supplements (see below).
Hungry for recipes that are friendly for GLP-1 medications? Grab my free recipe pack here.

Targeted supplements:
Data indicates that calorie intake reduces by 16-39% while taking a GLP1 medication (Spreckley 2026). Given this, dietary supplements may no longer be optional for many people (Johnson 2025). Supplements may include a mulvitamin/mineral supplement, supplements for muscle support and certain probiotics. You can speak to your dietitian about what supplements are right for you.
-
Looking beyond just protein
Protein is essential—but is not the whole story. As well, excessive dietary protein that is above the needs for repair or growth can be converted to fat by the liver and increase visceral adiposity (Mozafariun et al 2025).
Also include:
- Fiber-rich foods found in whole grains, beans, lentils, fruits, vegetables. Experts now specify the following fiber targets for those on a GLP-1: 25 g/day of fiber for women, 30 g/day for men and 35 g/day for those with diabetes (Sievenpiper et al 2026)
- Healthy fats found in olive oil, nuts, seeds, avocado, fatty fish
- Hydration: 2–3 L/day for digestion, bowel health, kidneys and energy, up to 4 L/day depending in climate and activity.
Balanced eating patterns (not just calorie tracking) support satiety, hormone balance, the microbiome, and metabolic health. When we focus on dietary patterns of foods to include, we can move beyond nutritional accounting and work with the natural properties of foods that work with our bodies to create satiety.
-
Building sustainable nutrition and lifestyle skills
GLP-1 medications aren’t a magic solution. They work best when combined with practical, sustainable health habits:
- Consistent meals with adequate protein, fiber, heathy fats and fluid
- Eating well consistently with meal planning and gentle prep ahead
- Strength training and aerobic activity each week.
- Stress management, emotional regulation, and good sleep (which improves GLP-1 effectiveness)
Social connection and mental health support also play important roles:
Working on skills around getting enough quantity and quality of sleep, managing stress and building skills in emotional regulation also help support nutrition skills.
- Poor sleep is associated with insulin resistance, increased hunger and weight increase. Poor sleep can reduce some of the benefits of GLP-1.
- Mental stress impacts the nervous system and elevates cortisol levels which promotes energy storage and invites food cravings for ultra-processed “comfort foods”. Some people cope with stress using substances such as alcohol or cannabis. GLP-1s help to reduce the impacts of chronic stress and help to alter food reward pathways in positive ways and may help reduce alcohol and other substance use disorders (Mozafarriun et al 2025).
Helping people develop strong social connections may help by reducing stress, increasing motivation and encouraging accountability (Mozafariun et al 2025).
Some more than others experience structural barriers to food, nutrition and lifestyle skills. These are called social determinants of health and require policy-level interventions. The majority of the true causes of obesity (a chronic, relapsing, remitting condition that impairs health) are not within an individual’s direct control.
-
Supporting a balanced relationship with food.
People who have struggled with their weight are also more at risk to have developed disordered eating, and maybe even eating disorders, as they pursue intentional weight loss. It is important that disordered eating is identified and treated through the addition of nutritional adequacy, building skills in eating well more consistently as well as in emotional regulation and improving body image and acceptance.
Disordered eating and eating disorders almost always begin with a diet and pursuing intentional weight loss. For many clients, connecting them with a psychologist is needed to address internalized weight bias, trauma, as well as psychological barriers to nutrition and lifestyle practices for self-care, as well as improving body image and acceptance.
Working with a registered dietitian and psychologist can help:
- Fuel your body with confidence
- Rebuild trust with hunger and fullness cues
- Address body image concerns
- Develop skills for emotional regulation
- Heal from trauma and internalized weight bias
- Receive help for mental health concerns.
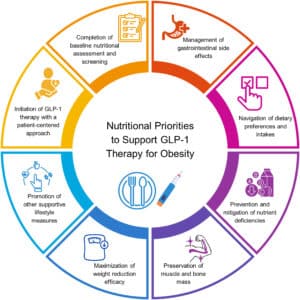
Image source: https://onlinelibrary.wiley.com/doi/10.1002/oby.24336
GLP-1s and “Food Noise”
One of the interesting impacts of the GLP1 medications is the reduction of what is called “food noise”, also known as food-related intrusive thoughts or food preoccupation (Mozafariun 2025). We can’t control the thoughts that we have, and so this experience of always thinking about food can be particularly distressing and agonizing for people.
Food noise also includes emotional eating, and external eating (eating in response to external triggers, regardless of hunger) (Mozafariun 2025) often showing up in the afternoon and/or evening.
Food noise is a controversial and hot topic. From an eating disorder perspective, food noise is a symptom of restricted food intake – a common scenario among people who are pursuing intentional weight loss. This phenomenon was observed in the famous Minnesota Starvation Diet, where men in WW2 concentration camps were starved and were noted to have intrusive food thoughts, among many other side effects.
This begs the question – what is the real problem – the food noise or the restriction which is fueling the food noise?
From an eating disorder perspective, the root driver of food noise is restrictive, disordered eating, which has many psychological and social underpinnings that also need to be addressed.
Regardless, the use of GLP-1s helps to reduce the experience of food noise, providing much relief from this distressing experience.
Supportive strategies to reduce food noise, regardless of GLP-1 use:
- Eat enough food throughout the day, especially early in the day—aiming to include protein-rich foods.
- Eat enough nutrition for the body you have today.
- Explore and address emotional and external eating cues
- Consider mindfulness-based eating or CBT to support behavior change
- Reflect on “wanting” (the desire for food) vs. physical hunger.
The use of GLP-1s has been found to reduce food cravings for high-fat foods, sugary foods and alcohol. GLP-1s also help reduce disordered eating including reduced emotional eating, less eating in response to external triggers, less binge eating, loss-of-control eating and food rumination. Some people are just less interested in food overall (Mozafariun 2025).
Some clients describe GLP-1s as slowing down their decision-making around food, making it easier to make intentional choices. The changed psychological experience helps to facilitate the changes that people are trying to make around food, nutrition and lifestyle.
Of note, some of these outcomes can be improved via mindfulness-based eating awareness training and practices. These observations also elucidate the complex neurobiology of food cravings. GLP-1 receptors are found throughout the body and within the brain and can have multi-system effects, including our reward-based eating. The GLP-1 receptors in the mesolimbic brain region are thought to help modulate reward behaviour.
What happens if I stop taking GLP-1s?
About 50-75%, up to 85% of people discontinue GLP-1s within 2 years—often due to cost, side effects, or preference. Unfortunately, most regain two-thirds of their lost weight within a year as well as worsening of metabolic health indicators (Mozaffarian et al., 2025; Khan et al., 2024) if nutritional and behavioural supports are not intensified (Sievenpiper 2026). This would seem to put people back into the viscous cycle of weight loss and regain.
More research is needed here around structured lifestyle programs to mitigate weight regain, including the addition of meal replacements. I am confident the pharmaceutical industry will not be funding these trials.
The nutrition and lifestyle skills described above are especially important if the person plans to stop using the GLP-1. A friendly reminder that while calorie restriction can achieve short-term reductions in weight (<12 months), it has not been shown to be sustainable long-term (>12 months). Calorie restriction appears to affect neurobiological pathways that control appetite, hunger, cravings and body weight, such that there is increased food intake and weight gain (Brown et al, 2022).
Is taking a GLP-1 the “easy way out”?
Absolutely not.
This myth reflects deep-rooted weight stigma. For many, GLP-1s provide a breakthrough after years of struggle. They don’t replace diet and lifestyle—they help people implement lasting changes. For some people, taking GLP-1s creates the mental space to be able to explore and address their food, nutrition and relationship with food.
Some clients tell me that, after taking a GLP-1, it is the first time *ever* in their life that they experienced the sensation of fullness. There is neurodiversity in our ability to feel hunger and to feel full. We don’t all feel these sensations the same way and at the same rate. If we didn’t live in a weight-biased world where people are trying to “control” their weight, this diversity wouldn’t be an issue.
We must move beyond the false dichotomy of “lifestyle vs. medication.” Both can work together to support health, quality of life, and autonomy.
Having compassion and empathy for a person whose experience is different from your own can go a long way to creating a safe space for us all to live, with the bodies and history that we have.
Final Thoughts & Nutrition Tips
Healthful eating is important for all people, regardless of body size, weight or health status (Brown et al, 2022). As Spreckley’s (2026) research found, GLP1 medications are effective for weight loss, a lack of appropriate nutrition oversight has lead to significant lean body mass loss and widespread nutritional deficiencies. Unmanaged GLP1 therapy has risks. Nutrition still matters while on a GLP1 therapy.

In midlife, it is important to get clear on the goals of nutrition and lifestyle interventions. Shift from restrictive dietary approaches to focusing on what the body needs to be healthy both physically, mentally and for overall well-being. We all have our own life story when it comes to our bodies, our weight, our relationship with food, movement, sleep and stress. There is no one size fits all approach to weight in midlife.
Focus on health, energy, and sustainability. Nutrition quality should be prioritized over restriction, especially in patients using GLP-1 therapies. The focus should be on providing the body with what it needs to be healthy, rather than eliminating foods like carbohydrates. A low carbohydrate diet is not needed on a GLP1 medication
There’s no “one size fits all” approach in midlife nutrition. If you’re taking Ozempic or a similar medication and need help with your eating, side effects, or lifestyle changes, reach out. A registered dietitian with GLP-1 experience can help you:
- Manage GI symptoms
- Build a GLP-1-friendly kitchen and routine
- Optimize your macronutrient and micronutrient intake
- Plan nourishing meals and snacks
- Adding in strategic supplements for your health
- Stay consistent, compassionate, and confident on your journey.

I have put together a collection of recipes to help you while taking a GLP-1 Medication. Click here to grab your copy!
References consulted in writing this blog post:
Jaime P Almandoz 1, Thomas A Wadden 2, Colleen Tewksbury 3, Caroline M Apovian 4, Angela Fitch 5, Jamy D Ard 6, Zhaoping Li 7, Jesse Richards 8, W Scott Butsch 9, Irina Jouravskaya 10, Kadie S Vanderman 11, Lisa M Neff 10. Nutritional considerations with antiobesity medications. Obesity (Silver Spring). 2024 Sep;32(9):1613-1631. doi: 10.1002/oby.24067. Available from: https://pubmed.ncbi.nlm.nih.gov/38853526/
Sandra Christensen 1, Katie Robinson 2, Sara Thomas 2, Dominique R Williams 2 Dietary intake by patients taking GLP-1 and dual GIP/GLP-1 receptor agonists: A narrative review and discussion of research needs. Obes Pillars. 2024 Jul 25:11:100121. Available from: https://pubmed.ncbi.nlm.nih.gov/39175746/
Brown J, Clarke C, Johnson Stoklossa C, Sievenpiper J. Canadian Adult Obesity Clinical Practice Guidelines: Medical Nutrition Therapy in Obesity Management. Available from: https://obesitycanada.ca/guidelines/nutrition, Accessed June 1, 2025.
Gallegos A. Fat loss vs weight loss: helping GLP-1 Patients focus on the right measurement. Medscape. April 2025. Available from: https://www.medscape.com/viewarticle/fat-loss-vs-weight-loss-helping-glp-1-patients-focus-right-2025a100085o?ecd=WNL_trdalrt_pos1_ous_250407_etid7344779&uac=81509PN&impID=7344779
Linda Gigliotti 1, Hope Warshaw 2, Alison Evert 3, Colleen Dawkins 4, Julie Schwartz 5, Caroline Susie 6, Robert Kushner 7, Savitha Subramanian 8, Deepa Handu 9, Mary Rozga 10 Incretin-Based Therapies and Lifestyle Interventions: The Evolving Role of Registered Dietitian Nutritionists in Obesity Care. J Acad Nutr Diet. 2025 Mar;125(3):408-421. Available from: https://pubmed.ncbi.nlm.nih.gov/39521378/
Brittany V B Johnson 1, Mary Milstead 1, Rachel Kreider 1, Rachel Jones 1 Dietary supplement considerations during glucagon-like Peptide-1 receptor agonist treatment: A narrative review. Obes Pillars. 2025 Sep 8:16:100209. doi: 10.1016/j.obpill.2025.100209.eCollection 2025 Dec. Available from: https://pubmed.ncbi.nlm.nih.gov/41368199/
Hall K. Physiology of the weight-loss plateau in response to diet restriction, GLP-1 receptor agonism and bariatric surgery. Obesity, vol 32(6): 1163-1168. https://onlinelibrary.wiley.com/doi/full/10.1002/oby.24027
Dariush Mozaffarian 1, Monica Agarwal 2, Monica Aggarwal 3, Lydia Alexander 4, Caroline M Apovian 5, Shagun Bindlish 6, Jonathan Bonnet 7, W Scott Butsch 8, Sandra Christensen 9, Eugenia Gianos 10, Mahima Gulati 11, Alka Gupta 12 13, Debbie Horn 14, Ryan M Kane 15 16, Jasdeep Saluja 17, Deepa Sannidhi 18, Fatima Cody Stanford 19 20, Emily A Callahan 1. Nutritional priorities to support GLP-1 therapy for obesity: A joint Advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society. Obesity (Silver Spring). 2025 May 30. doi: 10.1002/oby.24336. Online ahead of print. Available from: https://pubmed.ncbi.nlm.nih.gov/40445127/ and https://ajcn.nutrition.org/action/showPdf?pii=S0002-9165%2825%2900240-0
Schweitzer K. What to know about the WHO’s New GLP1 Guideline. Jan 2026. Available from: https://jamanetwork.com/journals/jama/article-abstract/2843811
J L Sievenpiper 1 2 3, J Ard 4, M Blüher 5, W Chen 6, J B Dixon 7, A Fitch 8, L Gigliotti 9, K Khunti 10, A Lecube 11 12, M E J Lean 13, B Mittendorfer 14, A F H Pfeiffer 15, D H Ryan 16, T Vilsbøll 17 18, L F Van Gaal 19. Nutritional and lifestyle supportive care recommendations for management of obesity with GLP-1 – based therapies: An expert consensus statement using a modified Delphi approach. Obes Pillars. 2025 Nov 11:17:100228 doi: 10.1016/j.obpill.2025.100228. Available from: https://pubmed.ncbi.nlm.nih.gov/41502845/
Spreckley M, Ruggiero CF, Brown A. Nutrition Strategies for Next-Generation Incretin Therapies: A Systematic Scoping Review of the Current Evidence Obesity Reviews, 2026. Jan 7:e70079. doi: 10.1111/obr.70079. Online ahead of print. https://pubmed.ncbi.nlm.nih.gov/41500509/
Elena Volpi Reza Nazemi, Satoshi Fujita Muscle tissue changes with aging – PMC. Curr Opin Clin Nutr Metab Care. Author manuscript; available in PMC: 2010 Jan 12. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2804956/
Tagged in: Calgary Dietitian, Calgary Nutritionist, GLP-1, Mediterranean diet, calgary dietician, health coach, healthy eating, weight loss, weight management


Welcome to the Energize Nutrition blog, where we share evidence-based nutrition content, designed to empower people’s midlife. Take a look around to find information on feeling your best.
If you need more individualized support, reach out to set up a free discovery call with Kristyn Hall.

Battling chronic hunger, poor energy, or inflammation? Discover what this powerful ingredient is and why it might be the solution!



{kind=link}